Hemp (from Old English
hænep) is a commonly used term for high-growing varieties of the
Cannabis
plant and its products, which include fiber, oil, and seed. Hemp is
refined into products such as hemp seed foods, hemp oil, wax, resin,
rope, cloth, pulp, paper, and fuel.
Other variants of the herb
Cannabis sativa
are widely used as a drug, commonly known as marijuana. These variants
are typically low-growing and have higher content of
tetrahydrocannabinol (THC). The legality of
Cannabis varies
widely from country to country, and from state to state in the United
States. In many countries regulatory limits for concentrations of
psychoactive drug compounds, particularly THC, in hemp require the use
of strains of the plant which are bred for low content.
[1]
Uses
Hemp grown for milk animal fodder.
Hemp
is used for many varieties of products including the manufacture of
cordage of varying tensile strength, durable clothing and nutritional
products. The
bast fibers can be used in 100% hemp products, but
are commonly blended with other organic fibers such as flax, cotton or
silk, for apparel and furnishings, most commonly at a 55%/45%
hemp/cotton blend. The inner two fibers of hemp are more woody and are
more often used in non-woven items and other industrial applications,
such as mulch, animal bedding and litter. The oil from the fruits
("seeds") oxidizes (commonly, though inaccurately, called "drying") to
become solid on exposure to air, similar to linseed oil, and is
sometimes used in the manufacture of oil-based paints, in creams as a
moisturizing agent, for cooking, and in plastics. Hemp seeds have been
used in bird feed mix as well.
[2] A survey in 2003 showed that more than 95% of hemp seed sold in the EU was used in animal and bird feed.
[3]
In
modern times hemp is used for industrial purposes including paper,
textiles, clothing, biodegradable plastics, construction (as with
Hempcrete and insulation), body products, health food and bio-fuel.
In
a new development hemp is being processed relatively inexpensively into
electrodes possibly even more efficient than graphene for use in
supercapacitors.
[4]
Food
Hemp seeds can be eaten raw, ground into a meal, sprouted, made into hemp milk (akin to soy milk), prepared as tea,
[5]
and used in baking. The fresh leaves can also be consumed in salads.
Products include cereals, frozen waffles, hemp milk ice cream, hemp
tofu, and nut butters. A few companies produce value added hemp seed
items that include the seed oils, whole hemp grain (which is sterilized
by law in the United States, where they import it from China and
Canada), dehulled hemp seed (the whole seed without the mineral rich
outer shell), hemp flour, hemp cake (a by-product of pressing the seed
for oil) and hemp protein powder. Even though hemp is marijuana's
cousin, hemp seeds contain no THC (tetrahydrocannabinol),
[citation needed] which is the psychoactive substance in marijuana.
Market share
Within
the UK, the Department for Environment, Food and Rural Affairs (Defra)
has treated hemp as purely a non-food crop. Seed appears on the UK
market as a legal food product, and cultivation licenses are available
for this purpose. In North America, hemp seed food products are sold,
typically in health food stores or through mail order. The United States
Department of Agriculture has concluded that "the market potential for
hemp seed as a food ingredient is unknown. However, it probably will
remain a small market, like those for sesame and poppy seeds."
[6] Since 2007 the commercial success of hemp food products has grown considerably.
[7][8]
Nutrition
Typical nutritional analysis
of hulled hemp seeds[citation needed] |
|---|
| Calories/100 g | 567 kcal |
|---|
| Protein | 30.6 |
|---|
| Carbohydrate | 10.9 |
|---|
| Dietary fiber | 6.0 |
|---|
| Fat | 47.2 |
|---|
| Saturated fat | 5.2 |
|---|
| Palmitic 16:0 | 3.4 |
|---|
| Stearic 18:0 | 1.5 |
|---|
| Monounsaturated fat | 5.8 |
|---|
| Oleic 18:1 (Omega-9) | 5.8 |
|---|
| Polyunsaturated fat | 36.2 |
|---|
| Linoleic 18:2 (Omega-6) | 27.6 |
|---|
| Linolenic 18:3 (Omega-3) | 8.7 |
|---|
| Gamma-Linolenic 18:3 (Omega-6) | 0.8 |
|---|
| Cholesterol | 0 mg |
|---|
| Moisture | 4.7 |
|---|
| Ash | 6.6 |
|---|
| Vitamin A (B-Carotene) | 4.0 IU/100g |
|---|
| Thiamine (Vit B1) | 1.4 mg |
|---|
| Riboflavin (Vit B2) | 0.3 mg |
|---|
| Pyridoxine (Vit B6) | 0.1 mg |
|---|
| Vitamin C | 1.0 mg |
|---|
| Vitamin E | 9.0 IU/100g |
|---|
| Sodium | 9.0 mg |
|---|
| Calcium | 74.0 mg |
|---|
| Iron | 4.7 mg |
|---|
Approximately
44% of the weight of hemp seed is edible oils, containing about 80%
essential fatty acids (EFAs); e.g., linoleic acid, omega-6 (LA, 55%),
alpha-linolenic acid, omega-3 (ALA, 22%), in addition to gamma-linolenic
acid, omega-6 (GLA, 1–4%) and stearidonic acid, omega-3 (SDA, 0–2%).
Proteins (including edestin) are the other major component (33%).
Hempseed's amino acid profile is comparable to other sources of protein
such as meat, milk, eggs and soy.
[9]
Protein
Digestibility Corrected Amino Acid Score values, which measure the
degree to which a food for humans is a "complete protein", were
0.49-0.53 for whole hemp seed, 0.46-0.51 for hemp seed meal, and
0.63-0.66 for dehulled hemp seed.
[10]
Hemp proteins thus have a PDCAAS equal to or greater than certain
grains, nuts, and some legumes. Soy protein, by comparison, has a PDCAAS
value of 1.0.
-
Japanese hemp seed seasoning
Swiss hemp beer uses blossoms
-
Storage
Hemp
oil, like any food oil rich in essential fatty acids, will
spontaneously oxidize and turn rancid within a short period of time if
not stored properly; Its shelf life is extended when stored in a dark
airtight container and refrigerated.
Fiber
Hemp stem showing fibers.
Hemp
fiber has been used extensively throughout history, with production
climaxing soon after being introduced to the New World. Items ranging
from rope, to fabrics, to industrial materials were made from hemp
fiber. Hemp was often used to make sail canvas, and the word
canvas derives from
cannabis.
[11][12] Today, a modest hemp fabric industry exists, and hemp fibers can be used in clothing.
[13] Pure hemp has a texture similar to linen.
[14]
Building material
Main article: hempcrete
Concrete-like
blocks made with hemp and lime have been used as an insulating material
for construction. Such blocks are not strong enough to be used for
structural elements; they must be supported by a brick, wood, or steel
frame.
[15] However hemp
fibres are extremely strong and durable and have been shown to be used
in replacement of wood for many jobs including creating very durable and
breathable homes.
The first example of the use of hempcrete was
in 1986 in France with the renovation of the Maison de la Turque in
Nogent-sur-Seine by the innovator Charles Rasetti.
[16] In the UK hemp lime was first used in 2000 for the construction of two test dwellings in Haverhill.
[17] Designed by Modece Architects,
[18]
who pioneered hemp's use in UK construction, the hemp houses were
monitored in comparison with other standard dwellings by BRE. Completed
in 2009, The Renewable House is one of the most technologically advanced
made from hemp-based materials.
[19] The first US home made of hemp-based materials was completed in August 2010 in Asheville, North Carolina.
[20]
A
panellized system of hemp-lime panels for use in building construction
is currently under test in a European Union funded research
collaboration lead by the University of Bath. The panels are being
designed to assure high quality construction, rapid on-site erection,
optimal hygrothermal performance from day one and energy and resource
efficient buildings. The 36 month long work programme aims to refine
product and manufacturing protocols, produce data for certification and
marketing, warranty, insurance cover and availability of finance. It
also includes the development of markets in Britain, France and Spain.
[21]
Hemp
is used as an internal plaster and is a mixture of hemp hurd (shive)
mixed with larger proportions of a lime based binder. Hemp plaster has
insulative qualities.
[22]
-
-
Hemp interior thermal insulation blocks
Hemp acoustic ceiling insulation
Concrete block made with hemp in France
Plastic and composite materials
Main article: Bioplastic
A mixture of fibreglass, hemp fiber, kenaf, and flax has been used since 2002 to make composite panels for automobiles.
[7][23]
The choice of which bast fiber to use is primarily based on cost and
availability. Various car makers are beginning to use hemp in their
cars, including Audi, BMW, Ford, GM, Chrysler, Honda, Iveco, Lotus,
Mercedes, Mitsubishi, Porsche, Saturn, Volkswagen
[24] and Volvo. For example, the Lotus Eco Elise
[25] and the Mercedes C-Class both contain hemp (up to 20 kg in each car in the case of the latter).
[26]
Hemp plastic interior of a car door
Hemp plastic automobile glove box
Hemp plastic column, automobile
Hemp composite sink basin
Paper
History and development
Wrapping paper with hemp fiber excavated from the Han Tomb of Wu Di (140-87 BC) at Baqiao, Xi'An.
The
first identified coarse paper, made from hemp, dates to the early
Western Han Dynasty, two hundred years before the nominal invention of
papermaking by Cai Lun, who improved and standardized paper production
using a range of inexpensive materials, including hemp ends,
approximately 2000 years ago.
[27] Recycled hemp clothing, rags and fishing nets were used as inputs for paper production.
The
Saint Petersburg, Russia paper mill of Goznak opened in 1818. It used
hemp as its main input material. Paper from the mill was used in the
printing of "bank notes, stamped paper, credit bills, postal stamps,
bonds, stocks, and other watermarked paper."
[28]
In
1916, U.S. Department of Agriculture chief scientists Lyster Hoxie
Dewey and Jason L. Merrill created paper made from hemp pulp and
concluded that paper from hemp hurds was "favorable in comparison with
those used with pulp wood."
[29][30] Modern research has not confirmed the positive finding about hemp hurds. They are only 32% and 38% cellulose.
[31]
On the other hand, hemp contains only 4-10% lignin against the 18-30%
found in wood. This lignin must be removed chemically and wood requires
more use of chemicals in the process.
[32]
The actual production of hemp fiber in the U.S continued to decline
until 1933 to around 500 tons/year. Between 1934-35, the cultivation of
hemp began to increase but still at a very low level and with no
significant increase of paper from hemp.
[33][34]
Contemporary
Hemp has never been used for commercial high-volume paper production due to its relatively high processing cost.
[citation needed] Currently there is a small niche market for hemp pulp, for example as cigarette paper.
[35]
Hemp fiber is mixed with fiber from other sources than hemp. In 1994
there was no significant production of 100% true hemp paper.
[36]
World hemp pulp production was believed to be around 120,000 tons per
year in 1991 which was about 0.05% of the world's annual pulp production
volume.
[37] The total world production of hemp fiber had in 2003 declined to about 60,000 from 80,000 tons.
[35] This can be compared to a typical pulp mill for wood fiber, which is never smaller than 250,000 tons per annum.
[36][38] The cost of hemp pulp is approximately six times that of wood pulp,
[37]
mostly because of the small size and outdated equipment of the few hemp
processing plants in the Western world, and because hemp is harvested
once a year (during August)
[citation needed]
and needs to be stored to feed the mill the whole year through. This
storage requires a lot of (mostly manual) handling of the bulky stalk
bundles. Another issue is that the entire hemp plant cannot be
economically prepared for paper production. While the wood products
industry uses nearly 100% of the fiber from harvested trees, only about
25% of the dried hemp stem — the bark, called bast — contains the long,
strong fibers desirable for paper production.
[39]
All this accounts for a high raw material cost. Hemp pulp is bleached
with hydrogen peroxide, a process today also commonly used for wood
pulp.
Market share
Around
the year 2000, the production quantity of flax and hemp pulp total
25000-30000 tons per year, having been produced from approximately
37000-45000 tonnes fibers. Up to 80% of the produced pulp is used for
specialty papers (including 95% of cigarette paper). Only about 20% hemp
fiber input goes into the standard pulp area and are here mostly in
lower quality (untreated oakum high shive content added) wood pulps.
With hemp pulp alone, the proportion of specialty papers probably at
about 99%. The market is considered saturated with little or no growth
in this area.
[40][41]
Jewelry
Main article: Hemp jewelry
Hemp
jewelry is the product of knotting hemp twine through the practice of
macramé. Hemp jewelry includes bracelets, necklaces, anklets, rings,
watches and other adornments. Some jewelry features beads made from
glass, stone, wood and bones. The hemp twine varies in thickness and
comes in a variety of colors. There are many different stitches used to
create hemp jewelry, however, the half knot and full knot stitches are
most common.
Cordage
Hemp
rope was used in the age of sailing ships, though the rope had to be
protected by tarring, since hemp rope has a propensity for breaking from
rot, as the capillary effect of the rope-woven fibers tended to hold
liquid at the interior, while seeming dry from the outside.
[42]
Tarring was a labor-intensive process, and earned sailors the nickname
"Jack Tar". Hemp rope was phased out when Manila, which does not require
tarring, became widely available. Manila is sometimes referred to as
Manila hemp, but is not related to hemp; it is abacá, a species of
banana.
Animal bedding
Hemp straw animal bedding.
Hemp
shives are the core of the stem, hemp hurds are broken parts of the
core. In the EU, they are used for animal bedding (horses, for
instance), or for horticultural mulch.
[43] Industrial hemp is much more profitable if both fibers and shives (or even seeds) can be used.
Water and soil purification
Hemp
can be used as a "mop crop" to clear impurities out of wastewater, such
as sewage effluent, excessive phosphorus from chicken litter, or other
unwanted substances or chemicals. Eco-technologist Dr. Keith Bolton from
Southern Cross University in Lismore, New South Wales, Australia, is a
leading researcher in this area. Hemp is being used to clean
contaminants at the Chernobyl nuclear disaster site. This is known as
phytoremediation - the process of clearing radioisotopes as well as a
variety of other toxins from the soil, water, and air.
[44]
Weed control
Main article: Weed control § Organic methods
The dense growth of hemp helps kill weeds, even thistle.
Hemp,
because of its height, dense foliage and its high planting density as a
crop, is a very effective and long used method of killing tough weeds
in farming by minimizing the pool of weed seeds of the soil.
[45]
Using hemp this way can help farmers avoid the use of herbicides, to
help gain organic certification and to gain the benefits of crop
rotation
per se. Due to its rapid, dense growth characteristics,
in some jurisdictions hemp is considered a prohibited noxious weed, much
like Scotch Broom. It has been used extensively to kill weeds in
agriculture.
Fuel
Biofuels,
such as biodiesel and alcohol fuel, can be made from the oils in hemp
seeds and stalks, and the fermentation of the plant as a whole,
respectively. Biodiesel produced from hemp is sometimes known as
"hempoline".
[46]
Filtered
hemp oil can be used directly to only power diesel engines. In 1892,
Rudolf Diesel invented the diesel engine, which he intended to fuel "by a
variety of fuels, especially vegetable and seed oils, which earlier
were used for oil lamps, i.e. the Argand lamp."
[47][48][49]
Production
of vehicle fuel from hemp is very small. Commercial biodiesel and
biogas is typically produced from cereals, coconuts, palmseeds and
cheaper raw materials like garbage, wastewater, dead plant and animal
material, animal feces and kitchen waste.
[50]
Cultivation
Hemp
is usually planted between March and May in the northern hemisphere,
between September and November in the southern hemisphere.
[51] It matures in about three to four months.
Millennia
of selective breeding have resulted in varieties that look quite
different. Also, breeding since circa 1930 has focused quite
specifically on producing strains which would perform very poorly as
sources of drug material. Hemp grown for fiber is planted closely,
resulting in tall, slender plants with long fibers. "Until the early
1900s industrial hemp was a valuable crop used all over the world for
its strong fibers and oil seeds. Today, however, the common perception
of the industrial hemp plant is generally negative and associated with
the drug marijuana. This perception is the legacy of a century of
powerful influences constructing hemp as a dangerous drug, even though
it is not a drug and it has the potential to be a profitable alternative
crop. In the United States, the public's perception of hemp as
marijuana has blocked hemp from becoming a useful crop and product,"
[52] in spite of its vital importance prior to World War II.
[53]
Ideally, according to Britain's Department for Environment, Food and
Rural Affairs, the herb should be desiccated and harvested towards the
end of flowering. This early cropping reduces the seed yield but
improves the fiber yield and quality.
[54] In these strains of industrial hemp the tetrahydrocannabinol (THC) content would have been very low.
[52]
The
seeds are sown from mid April to mid May with grain drills to 4–6 cm
sowing depth. Hemp needs less fertilizer than corn does. A total of
60–150 kg of nitrogen, 40–140 kg phosphorus (P
2O
5)
and 75–200 kg of potassium [5] per acre for hemp fiber made before
sowing and again later, maybe three to four weeks. When practiced,
especially in France double use of fiber and seed fertilization with
nitrogen doses up to 100 kg / ha rather low. Organic fertilizers such as
manure can utilize industrial hemp well. Neither weeds nor crop
protection measures are necessary.
[52]
Cultivars
Hemp strains USO-xx and Zolotoniski-xx
A total of 46 varieties of hemp with low levels of tetrahydrocannabinol (THC) are certified by the European Union (EU).
[55]
They have, unlike other types, a very high fiber content of 30-40%. In
contrast to cannabis for medical use, varieties grown for fiber and seed
have less than 0.2% THC and they are unsuitable for producing hashish
and marijuana.
[56] The most important cannabinoid in industrial hemp is cannabidiol (CBD) with a proportion of 1 to 5%.
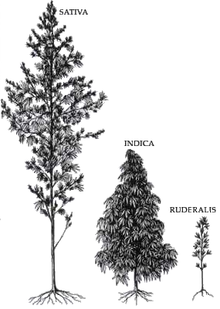
The variety of appearances for cannabis. Only C. sativa (left) is suited for industrial hemp, but it also has medicinal varieties.
Cannabis sativa L. subsp.
sativa var.
sativa is the variety grown for industrial use, while
C. sativa subsp.
indica
generally has poor fiber quality and is primarily used for recreational
and medicinal purposes. The major difference between the two types of
plants is the appearance and the amount of Δ
9-tetrahydrocannabinol
(THC) secreted in a resinous mixture by epidermal hairs called
glandular trichomes, although they can also be distinguished
genetically.
[57] Oilseed and fiber varieties of
Cannabis
approved for industrial hemp production produce only minute amounts of
this psychoactive drug, not enough for any physical or psychological
effects. Typically, hemp contains below 0.3% THC, while cultivars of
Cannabis grown for recreational use can contain anywhere from 2% to over 20%.
[58]
Harvesting
Industrial hempseed harvesting machine in France.
Smallholder
plots are usually harvested by hand. The plants are cut at 2 to 3 cm
above the soil and left on the ground to dry. Mechanical harvesting is
now common, using specially adapted cutter-binders or simpler cutters.
The cut hemp is laid in swathes to dry for up to four days. This was traditionally followed by
retting,
either water retting (the bundled hemp floats in water) or dew retting
(the hemp remains on the ground and is affected by the moisture in dew,
and by molds and bacterial action). Modern processes use steam and
machinery to separate the fiber, a process known as thermomechanical
pulping.
Location and crop rotation
For
profitable hemp farming, particularly deep, humus-rich, nutrient-rich
soil with controlled water flow is preferable. Water logged acidic,
compressed or extremely light (sandy) soils primarily affect the early
development of plants.
[citation needed]
Steep slopes and high altitudes of more than 400 m above sea level are
best avoided. Hemp is relatively insensitive to cold temperatures and
can withstand frost down to -5 degrees C.
[citation needed] Seeds can germinate down to 1-3 degrees.
[citation needed] Hemp needs a lot of heat, so earlier varieties come to maturation. The water requirement is 300-500 l / kg dry matter.
[citation needed]
Up to 3 feet growing roots into the soil can also use water supplies
from deeper soil layers. Worth noting is that the water requirement of
hemp is at least 14 times lower than that of cotton which takes between 7
000-29 000 l/kg, according to WWF.
[citation needed]
Hemp
benefits crops grown after it. For this reason it is generally grown
before winter cereals. Advantageous changes are high weed suppression,
soil loosening by the large hemp root system and the positive effect on
soil tilth. Since hemp is very self-compatible, it can also be grown
several years in a row in the same fields (monoculture).
Diseases
Main article: List of hemp diseases
Hemp
plants can be vulnerable to various pathogens, including bacteria,
fungi, nematodes, viruses and other miscellaneous pathogens. Such
diseases often lead to reduced fiber quality, stunted growth, and death
of the plant. These diseases rarely affect the yield of a hemp field, so
hemp production is not traditionally dependent on the use of
pesticides.
Environmental impact
Hemp is considered by a 1998 study in
Environmental Economics
to be environmentally friendly due to a decrease of land use and other
environmental impacts, indicating a possible decrease of ecological
footprint in a US context compared to typical benchmarks.
[59]
A 2010 study, however, that compared the production of paper
specifically from hemp and eucalyptus concluded that "industrial hemp
presents higher environmental impacts than eucalyptus paper"; however,
the article also highlights that "there is scope for improving
industrial hemp paper production".
[60] Hemp is also claimed to require few pesticides and no herbicides, and it has been called a carbon negative raw material.
[61][62]
Results indicate that high yield of hemp may require high total
nutrient levels (field plus fertilizer nutrients) similar to a high
yielding wheat crop.
[63]







 "The
available evidence suggests that removal of the prohibition against
possession itself (decriminalization) does not increase cannabis use.
... This prohibition inflicts harms directly and is costly. Unless it
can be shown that the removal of criminal penalties will increase use of
other harmful drugs, ... it is difficult to see what society gains."
"The
available evidence suggests that removal of the prohibition against
possession itself (decriminalization) does not increase cannabis use.
... This prohibition inflicts harms directly and is costly. Unless it
can be shown that the removal of criminal penalties will increase use of
other harmful drugs, ... it is difficult to see what society gains."

 One
of the most pernicious and ubiquitous effects of cannabis prohibition
is the conveyance of what traditionally should be law enforcement costs
and duties onto the public and private employers.
One
of the most pernicious and ubiquitous effects of cannabis prohibition
is the conveyance of what traditionally should be law enforcement costs
and duties onto the public and private employers.
 Evidence Supporting Marijuana's Medical Value
Evidence Supporting Marijuana's Medical Value